Last updated: March 10, 2020
| Translations Now Available: 日本語 (Japanese), Español (Spanish), 简体ä¸æ–‡ (Chinese (Simplified)), Français (French), Português (Portuguese (Brazil)) |
| Related FAQs:
|

Liana Zucco1, 2, Nadav Levy1, 2, Desire Ketchandji3, Mike Aziz3, Satya Krishna Ramachandran1
1. Beth Israel Deaconess Medical Center, Department of Anesthesia, Critical Care & Pain Medicine, Boston, USA
2. Healthcare Quality and Safety (MHQS) Program, Harvard Medical School, Boston, USA
3. Oregon Health & Science University, Department of Anesthesiology & Perioperative Medicine, Portland, Oregon, USA
Disclaimer: These guidelines were developed using the best judgement of clinicians with experience using anesthesia machines short-term in operating rooms. They are being frequently updated based on experience using anesthesia machines long-term for intensive care ventilation. The information and materials provided herein are provided only for information and educational purposes and do not establish a standard of care or constitute medical or legal advice. Readers are reminded to consult with their own institutions and medical/legal advisors.
![]() Disclaimer: The Anesthesia Patient Safety Foundation (APSF) is publishing this communication to help perioperative professionals in their management of patients with known or suspected 2019 novel coronavirus (COVID-19, also known as 2019-nCoV) infection. The 2019-nCoV outbreak is a rapidly evolving situation, so we strongly recommend following the Centers for Disease Control and Prevention updates on this topic.
Disclaimer: The Anesthesia Patient Safety Foundation (APSF) is publishing this communication to help perioperative professionals in their management of patients with known or suspected 2019 novel coronavirus (COVID-19, also known as 2019-nCoV) infection. The 2019-nCoV outbreak is a rapidly evolving situation, so we strongly recommend following the Centers for Disease Control and Prevention updates on this topic.
Introduction
The 2019 novel coronavirus (COVID-19, also known as 2019-nCoV) outbreak in Wuhan, China is rapidly approaching a pandemic as the number of countries with victims continues to grow. As of February 10, 2020, over 40,000 cases have been reported worldwide (REF: WHO situation reports). The fatality rate remains unknown, but a February 7, 2020 138-patient case series published in the Journal of the American Medical Association found a mortality rate of 4.3%1. With several documented cases of human-to-human transmissions2-5 2019-nCoV poses a high risk to all healthcare professionals in the perioperative setting.
We implore perioperative and hospital leaders to develop strategic steps for interventions on patients who have suspected or confirmed 2019-nCoV infection. The purpose of this communication is to present prudent safety measures in the perioperative setting, recognizing that these measures are based on learnings from previous viral outbreaks. Specifically, these measures were gleaned from successes and failures in curtailing transmission of the SARS-CoV and MERS-CoV in healthcare settings.5-7
2019-nCoV Pathogen Transmission
Pathogen transmission can occur via inhalation of infected respiratory droplets, in particular if the exposure of droplets is within close proximity (6 feet) and also includes contact with mucous membranes. It remains unclear if transmission can occur from direct or indirect contact with contaminated surfaces, however this may predispose to subsequent self-inoculation and/or transmission. It has been shown that another coronavirus, the SARS-CoV, was able to survive for 24 hours outside of the body, so at this time similar assumptions are being made regarding the 2019-nCoV.6, 7
Preventing transmission of the 2019-nCoV remains the most effective public health effort to lessen its impact. This effort involves rapid identification of cases, tracing of contacts, isolation/quarantine of infected/exposed individuals, and supportive care. Hospital-wide guidelines should be available for healthcare professionals to manage possible exposure to the virus in the perioperative setting in addition to the more commonly considered sites such as the emergency room, critical care units, and ambulatory clinics.
We recognize the perioperative setting as a site for possible unrecognized exposure to 2019-nCoV. It is therefore imperative to implement measures to mitigate perioperative transmission. As we learned from the SARS-CoV outbreak in 2002 in Toronto, nosocomial transmission represents a serious threat to health care systems and poses a significant burden on hospital systems and communities.7
What we learned from SARS-CoV and MERS-CoV outbreaks
The majority of SARS-CoV and MERS-CoV cases were associated with nosocomial transmission in hospitals7 and associated with the use of aerosol-generating procedures in patients with respiratory diseases. This places healthcare workers (HCW) including anesthesia professionals, intensivists, and nurses at a significant risk given the likelihood for a potential interface with droplets, sputum, or bodily fluids while performing routine procedures such as airway management.
During the outbreak of SARS-CoV in Toronto, despite existing safety protocols, half of all SARS-CoV cases were in HCWs, of which three died8. HCWs in Toronto that were at greatest risk of becoming infected were those involved in manipulating the airway or exposed to aerosolized pathogens via nebulizers, CPAP, BiPAP, or high flow nasal oxygen therapy. The SARS-CoV HCW infected cases from the Toronto outbreak occurred following the intubation of SARS-CoV infected patients on ICU, often when more than one attempt at intubation was required, and when more than three people were in the room.9, 10 Improved measures and adherence to PPE reduced transmission during the second SARS outbreak.
To protect and ensure the safety of health care workers and by extension patients by preventing nosocomial transmission of the novel coronavirus, a coordinated effort with full hospital support must be implemented.
Pathogen Transmission & the Anesthesia Work Environment
Within the operating room, the anesthesia work environment allows for numerous surfaces that can harbor droplets thus serving as reservoirs for the virus if proper droplet precautions or proper decontamination processes are not followed.
As noted previously, processes that favor aerosolization of sputum in infected and potentially infected individuals in the perioperative setting represents a potential source of exposure to HCW. For the anesthesia professional and intensivist, the time period which represents the highest risk of exposure involves direct contact with respiratory droplets during airway management primarily during intubation and extubation.11, 12 Furthermore, inadequate personal protective equipment (PPE), improper use of PPE, and poor hand hygiene are potential factors that can lead to transmission to the bedside HCW.13
Recommendations for Standard Practice in the Anesthesia Work Environment by APSF
As there are unconfirmed reports of transmission before symptoms are showing and given the rapid spread, it may be challenging to identify and isolate patients carrying the virus. We, therefore, recommend an escalation of standard of practice during airway management for all patients to reduce exposure to secretions.
Hand Hygiene:
Frequent hand washing is the single most important hygiene measure in protection against cross infection and must be actively enforced9. Alcohol -based hand wash gels should be located on or near every anesthesia workstation. Hand hygiene (HH) should be meticulously performed according to standard guidelines, specifically after removing gloves; after contact with soiled or contaminated areas; before touching the anesthesia machine, the anesthesia cart or its contents and after every contact with the patient (e.g.: placement of thermometer, nasogastric tube)
Personal Protective Equipment:
Personal protective equipment (PPE) should be available for all providers. Providers and their organizations should review protocols for correct donning and doffing PPE. Consider conducting mock intubation/extubation drills using PPE in a real environment (in situ). This is an opportunity to promote correct use of PPE among providers and to identify barriers to adherence. Consideration should be taken to avoid “rescue like†crash intubations where PPE cannot be fully adhered to, at the organizational level. We suggest a lowered threshold for planning elective or semi-elective intubations in relevant cases. Given the risk of transmission with non-invasive ventilation, we recommend proceeding early directly to endotracheal intubation in patients with acute respiratory failure.
N95 masks fulfill the filtering efficiency criteria of the National Institute for Occupational Safety and Health (NIOSH) and are approved for protection against droplet and airborne transmission of 95% of particles greater than 0.3 microns in size. N95 masks, which must be fit tested, are believed to offer protection against the contact and droplet spread of the coronavirus. At a minimum, N95 masks should be used for all known or suspected cases of 2019-nCoV, as well as for any asymptomatic “open airway’’ cases, e.g.: interventional pulmonology procedures. A powered air-purifying respirator (PAPR) provides superior protection and may be warranted for airway procedures in patients with known or suspected 2019-nCov given prior cases of HCW infection with SARS-CoV using N95 masks.
Disposable OR caps and beard covers should be properly worn to reduce the risk of contaminating hands by touching hair which may have been exposed to droplets. Disposable fluid-resistant long-sleeved gowns, goggles and disposable full-face shields are recommended for frontline medical staff at risk of exposure. Hand washing is essential before and after donning or doffing PPE.
Airway manipulation (Intubation and Extubation):
Prior to intubation, protect yourself by donning the appropriate gloves, facemask/PAPR, eye shield and gown. Prepare your intubating equipment next to the patient, and plan for its disposal, in order to limit the distance of travel of contaminated equipment. Use double gloving technique during intubation. Use the outer gloves to sheath the laryngoscope blade and change the inner gloves as soon as possible afterward.11
During extubation maintain strict HH, wear a mask with a face shield and carefully dispose of contaminated equipment. Limit the number of staff members present for intubations/extubations to reduce the risk of unnecessary exposure.
Strongly consider prophylactic antiemetics to reduce the risk of vomiting and possible viral spread.9
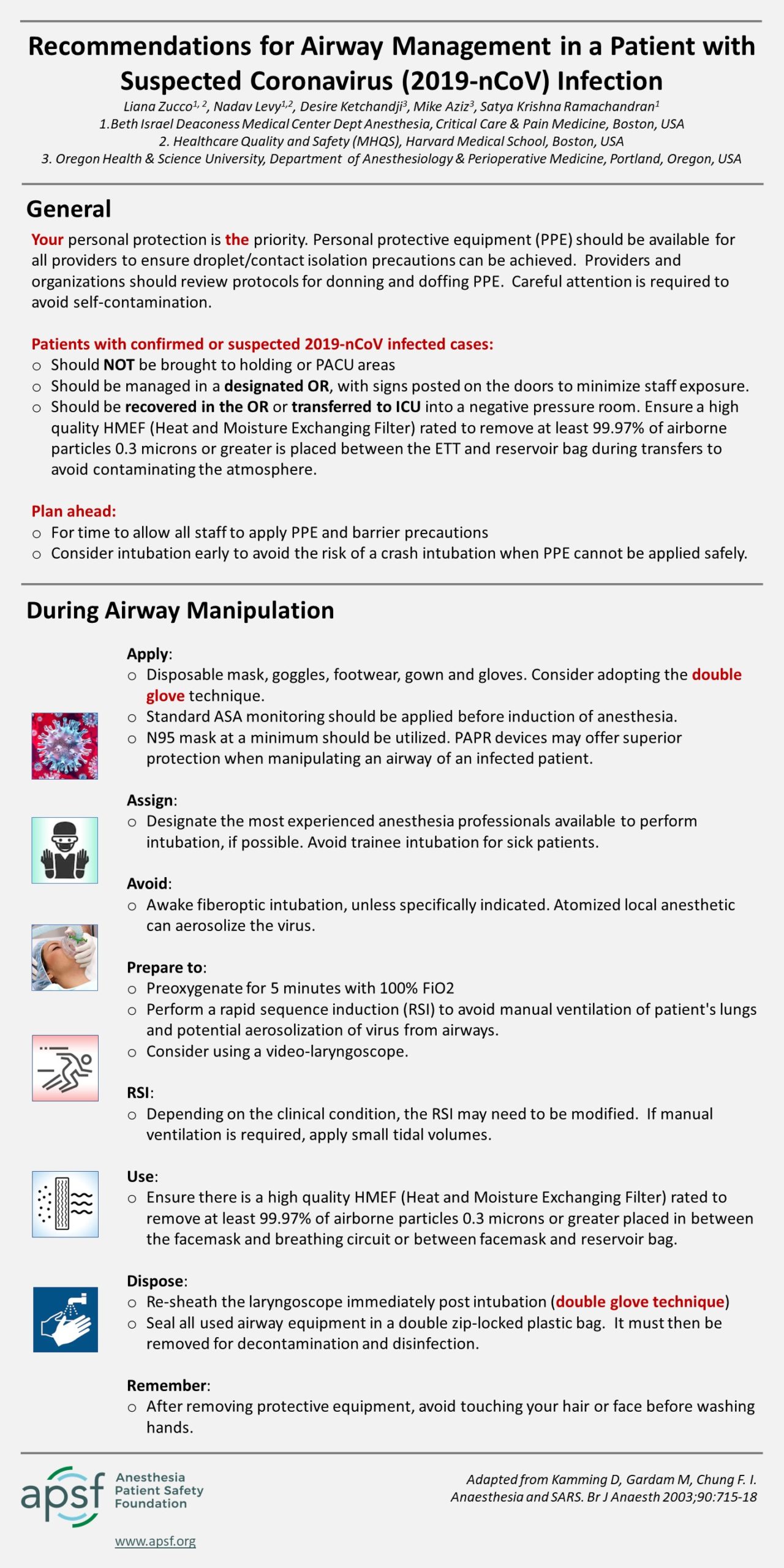
Recommendations for Airway Management in a Patient with Suspected Coronavirus (2019-nCoV) Infection
Adapted from: Kamming, Gardam and Chang; BJA 2003
General Precautions:
- Confirmed or suspected 2019-nCoV infected cases should NOT be brought to holding or PACU areas. A designated OR should be allocated for such cases and signs posted on the doors to minimize staff exposure. Infected cases should be recovered in the operating room or transferred to ICU into a negative pressure room. Ensure a high quality HMEF (Heat and Moisture Exchanging Filter) rated to remove at least 99.97% of airborne particles 0.3 microns or greater is placed between the endotracheal tube and reservoir bag during transfers to avoid contaminating the atmosphere.
- YOUR personal protection is a priority. Personal protective equipment (PPE) should be available to all providers to ensure airborne/droplet/contact isolation precautions can be achieved. Plan ahead in order to allow sufficient time for staff to apply PPE and barrier precautions. Careful attention is required to avoid self-contamination.
During Airway Manipulation:
- Apply a fit-tested disposable N95 respirator or a Powered Air-Purifying Respirator (PAPRs), goggles, gowns, gloves and protective footwear. Apply the double glove technique. Apply standard monitoring to the patient, as you would for any induction of anesthesia.
- Designate the most experienced anesthesia professional available to perform intubation, if possible. Avoid trainee intubations of sick patients during this time.
- Avoid awake fiberoptic intubation unless specifically indicated. Atomized local anesthetic will aerosolize the virus. Consider using a video-laryngoscope to improve intubation success.
- Prepare to preoxygenate for a minimum of 5 minutes with 100% oxygen and perform a rapid sequence induction (RSI) in order to avoid manual ventilation of patient’s lungs and potential aerosolization of virus from airways.
- Perform an RSI (ensure a skilled assistant is available to perform cricoid pressure) or a modified RSI as clinically indicated. If manual ventilation is required, apply small tidal volumes.
- Ensure the placement of a high quality HMEF (Heat and Moisture Exchanging Filter) rated to remove at least 99.97% of airborne particles 0.3 microns or greater in between the facemask and breathing circuit or in between facemask and reservoir bag.
- Re-sheath the laryngoscope immediately post intubation (double glove technique). Seal ALL used airway equipment in a double zip-locked plastic bag. It must then be removed for decontamination and disinfection.
- After removing protective equipment, remember to avoid touching your hair or face before washing hands.